
The importance of ankle mobility is paramount in the squat – in fact, any closed chain movement where the foot is in contact with the ground.
Dorsi-flexion of the ankle (ie: lifting the ball of the foot with the heel in contact with the ground) is perhaps the most important of the degrees of freedom at the ankle. Movement of this type allows for the tibia (shin) to move forward relative to the foot. This is necessary directly for correct body positioning and indirectly for efficient production and maximisation of force.
Anatomy:
Let’s first examine the anatomy behind ankle dorsi-flexion. The image below shows the posterior musculature of the lower limb. The superficial two-headed muscle below the posterior of the knee is the gastrocnemius. This biarticular muscle (runs over two joints) attaches to the Achilles tendon which attaches to the heel (calcaneus). Also attaching to the Achilles tendon is the soleus, the deeper of the two muscles in the illustration below. All three structures are involved in plantar flexion of the ankle, and thus, should any of these three structures (gastroc., soleus, or Achilles tendon) be short or tight, it limits the ability to achieve dorsi-flexion (indicated by the arrow).

Effects of Poor Ankle Dorsi-flexion:
Failure to achieve sufficient ankle dorsi-flexion will either cause the absolute inability to complete a movement, or will create a flow-on effect up the chain causing injurious situations in the knee and lumbar spine.
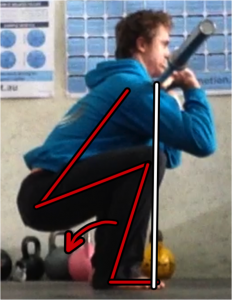
Let’s case study this flow-on effect. The two images below illustrate the systemic upchain changes in body position as a result of limited dorsi-flexion of the ankle. The figure on the left shows limited ankle dorsiflexion. The figure on the right shows more favourable dorsiflexion.


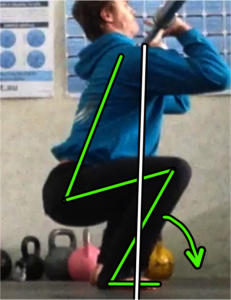
As a result of this immobility, the following negative biomechanical chain of effects results:
- The tibia is dragged to a more vertical position by the gastocs. and soleus (by way of the Achilles tendon).
- This shifts the distal end of the femur backwards, and by association, the proximal end (the hip).
- With the pelvis posteriorly displaced, the trunk inclines forward. Without this forward inclination, the centre of gravity would fall outside the base of support. As long as your centre of gravity falls within your base of support you can maintain an upright stance. If it leaves your base of support, to prevent falling you must bring it back by either increasing the base of support or moving your centre of gravity back inside. Increasing the base of suport is not an option, so the only strategy to maintain stance is to shift the centre of gravity forward – hence the forward inclination of the trunk.
- The forward inclination of the trunk often results in a loss of neutral spine (as demonstrated in the first image), impairing the ability to transfer force from the hips to the load.
- With the torso less upright, a greater degree of thoracic mobility and shoulder mobility (flexion of the shoulder) is required to rack the bar on the anterior deltoids (front of shoulder). This is demonstrated in the contrasting images – shoulder flexion is almost identical in both, but the lack of thoracic extension and the angle of the torso make it difficult to achieve an effective rack position.
- This leads in turn to an anterior shift of the bar relative to the base of support. The increase in this moment arm increases the torque applied by the load, effectively lengthening the lever, and increases the subsequent requirement of the body to produce a greater force for a given load.

Practical Implications:
So what are the practical implications of poor dorsi-flexion of the ankle? Primarily, it leads to a reduced force generating ability – less strength – particularly in the front squat (and therefore clean) and overhead squat (and therefore snatch). In lighter or unweighted versions of these movements, loss of technique and unsafe joint loading patterns leak efficiency (reducing work capacity) and increase the risk of injury. Complex single limb movements such as pistols are particularly exposed by poor ankle dorsi-flexion.
The use of a lifting shoe with a raised heel effectively reduces the need for ankle dorsi-flexion, relative to the size of the heel wedge. Although this technique should be used to maximise force generation, it is not an acceptible long term strategy to hide immobility.
Action plan:
Due to the high ratio of tendon to muscle in the lower leg, increasing dorsi-flexion of the ankle is a long term prospect. Non-the-less, the following initiatives can and should be taken:
- Deep tissue mobilisation of the gastrocs. and soleus (using trigger point balls, foam rollers and barbell rolling). These mobilisations should be completed with the toes pointed.
- PNF of the gastrocs. and soleus to increase useable length and shift to a more favourable length-tension relationship (increasing not only muscle length, but force generating capacity).
- Simply spend as much time as possible in ankle dorsi-flexion. Make sure you’re doing this with knee bent and knee straight.



